As you know, exercise can have numerous benefits in preventing and treating an array of chronic diseases, one of these being Osteoporosis. Osteoporosis is characterized by low bone mass and deterioration of bone tissue leading to compromised bone strength, which predisposes an individual to an increased risk of fracture. Similarly, osteopenia is a term used to describe low bone density compared to the standard, however it is not considered a disease, or as severe as osteoporosis.
4.74 million Australians over 50 years of age (66%) have osteoporosis or osteopenia, while it is projected that by 2022, there will be 6.2 million Australians over the age of 50 with one of these conditions, a 31% increase (1). Osteoporosis is considered a ‘silent disease’ due to the fact that as many as 4 out of 5 people with osteoporosis don’t know they even have the condition even though they are at an increased risk of bone fracture. Hence, the real enemy is really the fractures that occur at a greater incidence due to Osteoporosis.
While less than 5% of falls result in fracture, over 90% of fractures result from a fall. In 2013, one fracture occurred ever 3.4 minutes in Australia (394 per day), while by 2022 it is projected that a fracture will occur once every 2.9 minutes (501 per day). Globally, 1 in 3 women and 1 in 5 men aged over 50 will experience osteoporotic fractures (1). There are several reasons as to why women have a greater likelihood of fracture, which include: a lower peak bone mass, smaller bones, experiencing greater cortical thinning (loss of outside portion of bone), bone loss due to the reduction in oestrogen associated with menopause, and finally the fact that women tend to live longer and thus have more time for a fracture to occur.
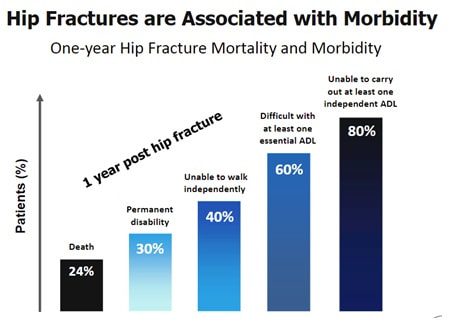
Of all osteoporotic fractures in Australia, 46% are vertebral (most common), 16% are hip (most devastating) and 16% are wrist. There is a cascade effect with fractures, this being that the risk of fracture rises with each new fracture. Following a fracture, there is a 2-4 fold increase in the risk of subsequent fracture, while women who suffer a spinal fracture are >4 times more likely to have another fracture within the next year. Hip fractures have a significant link to mortality and morbidity, as 24% of patients 1 year post fracture have deceased, while 80% are unable to carry out at least one independent activity of daily living (2).
As you know, exercise can have numerous benefits in preventing and treating an array of chronic diseases, one of these being Osteoporosis. Osteoporosis is characterized by low bone mass and deterioration of bone tissue leading to compromised bone strength, which predisposes an individual to an increased risk of fracture. Similarly, osteopenia is a term used to describe low bone density compared to the standard, however it is not considered a disease, or as severe as osteoporosis.
4.74 million Australians over 50 years of age (66%) have osteoporosis or osteopenia, while it is projected that by 2022, there will be 6.2 million Australians over the age of 50 with one of these conditions, a 31% increase (1). Osteoporosis is considered a ‘silent disease’ due to the fact that as many as 4 out of 5 people with osteoporosis don’t know they even have the condition even though they are at an increased risk of bone fracture. Hence, the real enemy is really the fractures that occur at a greater incidence due to Osteoporosis.
While less than 5% of falls result in fracture, over 90% of fractures result from a fall. In 2013, one fracture occurred ever 3.4 minutes in Australia (394 per day), while by 2022 it is projected that a fracture will occur once every 2.9 minutes (501 per day). Globally, 1 in 3 women and 1 in 5 men aged over 50 will experience osteoporotic fractures (1). There are several reasons as to why women have a greater likelihood of fracture, which include: a lower peak bone mass, smaller bones, experiencing greater cortical thinning (loss of outside portion of bone), bone loss due to the reduction in oestrogen associated with menopause, and finally the fact that women tend to live longer and thus have more time for a fracture to occur.
Of all osteoporotic fractures in Australia, 46% are vertebral (most common), 16% are hip (most devastating) and 16% are wrist. There is a cascade effect with fractures, this being that the risk of fracture rises with each new fracture. Following a fracture, there is a 2-4 fold increase in the risk of subsequent fracture, while women who suffer a spinal fracture are >4 times more likely to have another fracture within the next year. Hip fractures have a significant link to mortality and morbidity, as 24% of patients 1 year post fracture have deceased, while 80% are unable to carry out at least one independent activity of daily living (2).
Three ways to reduce the risk of developing osteoporosis and potential subsequent fractures include:
- Maximise peak bone mass – Achieved around the age of 20-30yrs. A 10% increase in PBM may delay the development of osteoporosis for 13 years
- Prevent or slow bone loss – A 1 SD reduction in BMD increases the risk of hip fracture by 2-3 fold
So how YOU do this?
Bone is a dynamic tissue and therefore adapts to the stress placed on it. The biggest modifiable risk factor for osteoporosis is physical inactivity, and thus exercise is ‘bone building’ and leads to maximising peak bone mass, prevention of age-related bone loss and prevention of falls due to improved strength and balance (3). This phenomenon is explained by osteocytes; strain-sensitive cells that respond to the stresses placed on bone and stimulate osteoblasts (bone-building cells) to form bone. Hence, exercise can be used to maximise bone strength and prevent the onset of osteoporosis, while it can manage already diagnosed osteoporosis by improving bone mineral density and reducing falls risk. It is also associated with improved outcomes following a fracture (4).
Moderate to high impact weight bearing activities which vary in direction can maintain or increase bone mineral density in older adults by 1-3%. Additionally, targeted (hip and spine muscles), high intensity (70-85% max) progressive resistance training can also have the same effect (5). Hence, a multi-modal program incorporating both weight-bearing impact activities plus PRT has been shown to be most effective for improving BMD and reducing the risk of osteoporosis or fracture. It is recommended that on 4-7 days of the week we complete 50 jumps (weight bearing exercise) to maximise bone mineral density (5).
Furthermore, you must also challenge your balance which will help minimise your risk of falls. For high risk individuals (previous fracture or osteoporosis), activities to avoid include those with twisting and/or forward flexion with loading of the spine (e.g. sit-ups). Finally, complementing exercise with adequate dietary intake of vitamin D and calcium is shown to be a modifiable risk factor that can reduce risk of osteoporosis.
At Inspire Fitness for Wellbeing our Exercise Physiologists work to prevent and manage an array of chronic diseases such as osteoporosis. Our design of individually targeted exercise programs will help minimise the risk of developing such conditions, while we may also help treat an already diagnosed condition.
If this applies to you, please contact us on 9857 3007 to speak to an Exercise Physiologist about introducing beneficial physical activity into your lifestyle!
References:
1. Watts JJ, Abimanyi-Ochom J, Sanders KM. Osteoporosis costing all Australian: a new burden of disease analysis-2012 to 2022.
2. Lu-Yao GL, Baron JA, Barrett JA, Fisher ES. Treatment and survival among elderly Americans with hip fractures: a population-based study. American Journal of Public Health. 1994 Aug;84(8):1287-91.
3. Sinaki M. Exercise and osteoporosis. Archives of physical medicine and rehabilitation. 1989 Mar;70(3):220-9.
4. Singh NA, Quine S, Clemson LM, Williams EJ, Williamson DA, Stavrinos TM, Grady JN, Perry TJ, Lloyd BD, Smith EU, Singh MA. Effects of high-intensity progressive resistance training and targeted multidisciplinary treatment of frailty on mortality and nursing home admissions after hip fracture: a randomized controlled trial. Journal of the American Medical Directors Association. 2012 Jan 1;13(1):24-30.
5. Beck BR, Daly RM, Singh MA, Taaffe DR. Exercise and Sports Science Australia (ESSA) position statement on exercise prescription for the prevention and management of osteoporosis. Journal of science and medicine in sport. 2017 May 1;20(5):438-45.

 RSS Feed
RSS Feed
